
Why Hospitality Matters in Healthcare
A diagnosis & treatment plan for care delivery
Great Patients Think Alike
Not to brag, but I’m a really good patient. Like, the teacher’s pet of patients. I come prepared for appointments, I follow my treatment plans, and I bring a bottle of wine around the holidays.
I met my co-founder Chloe through a friend, who, having heard us each talk ad nauseam about being “professional patients,” thought we might deserve each other and set us up on a blind friend date. Over an oat milk latte (me) and green tea (her), we talked shop. We shared our hospital horror stories. We traded specialist recommendations. And we admitted that there was more to the doctor’s pet game than just vying to be the favorite patient — it was about feeling some agency over the process. Being the perfect patient could, at best, make us stand out enough to “earn” more attention from our practitioners, and at worst, fill in the gaps our doctors didn’t have the time or energy to fill.
The conversation quickly turned to how we were craving a doctor’s office that just “got it.” We had both gotten sucked into the healthcare system at a relatively young age. Though the autoimmune world (mine) and the cancer world (hers) didn’t overlap much, we were both left fantasizing about a place that could do it all.
Fast forward six months, and we were pitching a new kind of doctor’s office we thought could do just that: a primary care members club called The Lanby. We said our mission was two-fold: A+ care (excellent, comprehensive medicine & wellness), and A+ delivery (high-touch, hospitality-driven patient experience). And while nobody disagreed with the premise of A+ care, I found that we were getting pushback on the value of A+ delivery over, and over, and over again.
People typically don’t associate healthcare with good service. Providers see it as gratuitous, even a distraction, and patients have become resigned to DMV-level treatment at the doctor’s office. We’ve sort of come to accept that this is the way things are. But how we deliver care has just as big an impact on health outcomes as what we’re delivering. In fact, bad delivery might be the biggest barrier standing between us and our health. It’s time to hold the doctor’s office to a higher standard.
What follows is a defense of A+ delivery in three questions:
- Why is the patient experience so bad?
- Why does that matter for our health?
- How can we leverage hospitality to get to A+ delivery?
Healthcare’s Customer Service Problem
Good customer service is about more than a friendly front desk — it’s about servicing the customer. It’s the implementation of features that make the service easier, more efficient, more effective, more transparent, more personalized, and overall better to use.
With that in mind, this is the customer service we’ve become accustomed to in healthcare: impenetrable staff, intimidating practitioners, paper files, paper robes, long waits, short visits, very-80s patient portals, depressing offices, lack of access to our own data, opaque pricing…the list goes on. The healthcare system is signaling to the patient at every touchpoint that, pretty much, you can take it or leave it. As investor Bill Gurley puts it, “[T]he U.S. healthcare market is the least customer centric of any customer service industry…We are so numb to the pain, that we rarely object or complain, and the doctor’s indifference to the consumer’s time is so common and widespread, that it is a frequent meme in jokes and cartoons.”¹ The healthcare industry is, at its core, a service industry, so how did this service get so bad?
The reality is, healthcare’s customer service problem is actually a consumer service problem. While a patient may be the consumer of the service, she’s far from the traditional customer:
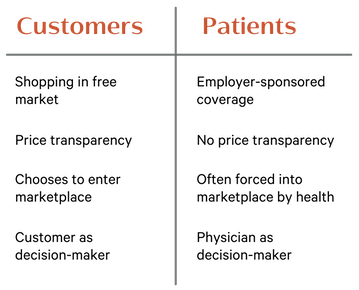
Patients find themselves in this strange position in large part due to the way our healthcare system was designed. The American employer-sponsored model is something of a World War II relic, developed in response to the Stabilization Act of 1942’s mandated national wage freeze.² It’s a piecemeal, reactionary, uniquely³ inefficient system with many power-wielding stakeholders that aren’t the patient, including employers, insurance companies, and large hospital networks.
Up against these forces, the patient always loses out. As healthcare founder Nick Soman explains, “When traditional health insurance companies propose new rates to regulators each year, they are governed by a medical loss ratio: they have to spend 80% of the premiums they charge on care, and can hold up to 20% back to cover administrative costs and profit.” In other words, as healthcare costs go up, every stakeholder profits but the patient.
Bill Gurley aptly describes how this model, in turn, impacts provider incentives:
If you were a U.S. healthcare provider, who would you view as the customer? The employer bears the eventual costs. The insurance carriers process the payment. The employee uses the service, but they did not chose you based on the prices of your services, and you never discussed or disclosed price to them. Those prices were negotiated between you and the different carriers that placed you on the various plans chosen by the employer. As you can see, its not unreasonable that, as a provider, you would not actually view the employee that utilizes your services as the customer. They are far from your only constituent in the system, and they are absolutely NOT the party that is paying the bill or negotiating price.⁵
So by the time you’re at the doctor’s office, even though you might feel like you’re the customer, the doctor is only acting rationally in not treating you like one. And that means normal customer service rules and incentives don’t apply. Which is how today, a staggering 96% of patient complaints are about service (versus 4% about the care itself).⁶
This isn’t just unpleasant — it’s bad for our health.
Bad Service Is Bad For You, Too
Without good systems for delivery, health outcomes suffer. If we walk through the patient experience under the traditional fee-for-service model, we can see where service falls short, and how that impacts our health:
Booking the visit
No good service makes you wait weeks to access it. This should be especially true when that service is healthcare. But a new primary care patient waits an average of 21.7 days⁷ for an appointment, and existing patients don’t fare much better (my own most recent wait time was 18 days). It’s not that there aren’t ways to reduce this time. Service industries, including some healthcare providers, have successfully implemented practices that improve appointment access, including holding back next-day appointments, limiting booking windows to 30 days, and using telemedicine to triage urgent issues. But physicians under a fee-for-service model have to prioritize volume over quantity, so incentives aren’t aligned in a way that encourages implementation.
Bad hold music aside, the real booking problem is that in the face of a 21-day wait for an appointment, a patient is left with three bad options:
- Defer treatment entirely: This is not great for health outcomes, for obvious reasons.
- Take the appointment: This is a more contained version of the above. Taking the appointment in three weeks means taking the bet that your symptom won’t significantly worsen in that time. The bet that your cough doesn’t progress into bronchitis, that rash doesn’t spread, or the injury that should be immobilized just gets way more painful. If I’m calling my doctor, I usually don’t have a symptom I’m interested in waiting weeks to sort out. Which is how so many of us end up going with Option 3.
- Opt for urgent care: If primary care is the produce section, urgent care is the frozen foods aisle. Frozen may be faster, but fresh is better. Unfortunately, quick fixes don’t yield better outcomes and lead to unnecessary treatment.⁸ Urgent care also pulls patients out from their continuum of care. Since notes from those visits rarely end up getting back to the PCP, a patient’s health narrative ends up being told across different files in different places, allowing important information to slip through the cracks.
The visit itself
Optimal care delivery is the result of a successful partnership between patient and practitioner. The patient brings the lived experience of his symptom, along with information about the genetic, family history, and lifestyle factors that may be contributing to the presented symptom. The doctor brings medical expertise and the professional experience of having seen similar cases. The optimal doctor’s office experience is one that facilitates seamless communication between partners.
Instead, by the time the patient and doctor reach the exam room, each partner is bringing a fair amount of baggage to the table:
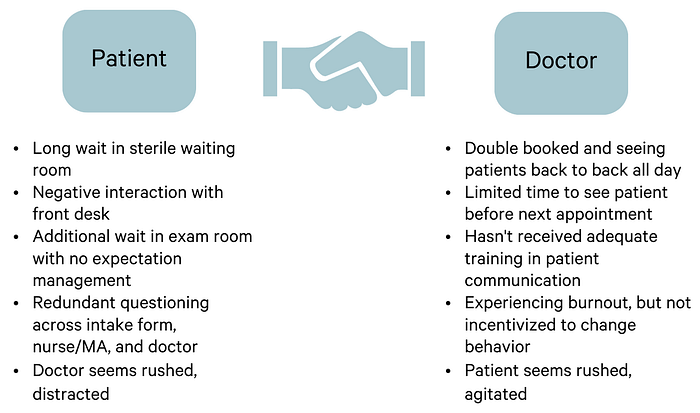
The average primary care appointment lasts 15 minutes⁹ (one of the more generous stats I found, though I’ve seen numbers as low as 8 and 11). Without the time or the bandwidth, doctors miss out on the information needed to diagnose or treat, and the opportunity to shore up the patient trust needed to get that information. Instead, “[r]unning late and decision fatigue” push physicians towards more reactionary, unpersonalized care. A doctor is 26% more likely to prescribe an antibiotic at 4 pm than at 8 am for the same kind of patient with the same issue.¹⁰
In this tight window, preventive care inevitably gets the shaft. This oversight has perhaps the biggest impact of all on our health: up to 40% of annual deaths caused by the top five causes of death in the U.S. are preventable.¹¹ The results of a model that pushes physicians to prioritize reaction over proaction are, in a word, deadly. And when we take an even bigger step back, the harm starts before the visit ever takes place, because it’s a model designed to push patients away.
Patient buy-in
As patients, we know what it’s like to go through all of the above, so we avoid the doctor unless we feel like we really have to go. We skip annuals, we don’t get our blood work done, and when our doctor tells us we should probably come back in three months to check on that thing, we don’t. While there are plenty of compelling, well-studied, life-or-death reasons to actively seek out preventive care, so many of us still think of “preventive” as a buzzword for biohackers with the luxury of time.
A patient culture built around ignoring the doctor for as long as possible leads to immeasurable lost opportunity to provide “upstream” care, not to mention unnecessarily high health care bills.¹² If prevention is the gold standard, how can we get patients through the door before they’re already sick?
This is where the idea of A+ delivery comes in. Making the process easier might get us to do something we think we need to. But the superpower of excellent service, true A+ delivery, is its ability to flip that switch in our minds from “need” to “want”. Once we want something, we tend to do two things: 1. Realize how much we actually did need that thing (a rare time we like confirmation bias); 2. Use it.
At The Lanby, we knew that getting to A+ was going to take more than just better customer service. Good customer service gets you to tolerable, “no complaints” healthcare, but it doesn’t get you to the next level: what I’ve often thought of as “Michelin-worthy” healthcare. If The Lanby was going to be an experiment in switch flipping, we had to provide hospitality.
Healthcare Hospitality
In Setting The Table, legendary restaurateur Danny Meyer, who I have always maintained would run the best hospital, says, “Hospitality is present when something happens for you. It is absent when something happens to you.”¹³ If the problem of A+ delivery can be described as flipping the switch from “need” to “want”, perhaps the solution can be found in flipping the switch from “to” to “for”.
As a hospitality-driven practice, we’re committed to doing things for our patients instead of to them. That means treating patients with a renewed curiosity and attentiveness, finding ways to take the work out of wellness, and taking pride in going the extra mile. To get there, we translated the principles of Michelin-star service into a new language, for a new setting, and with a different goal: hospitable healthcare.
Here are the central tenets of our healthcare hospitality philosophy:
- Follow the golden rule. Patients are entrusting you with their most precious resource (their health), so treat them the way you would hope to be treated at the doctor’s office.
- Help set clear expectations. This is not a subway track — if we’re running a few minutes behind, nobody wins when we keep that information to ourselves.
- Be an active, empathetic listener. Each case is a medical investigation. Ask good questions to get good clues. No detail is too small — if the patient didn’t think it was important, she wouldn’t have brought it up.
- Visit notes aren’t just for the doctor. Everyone who interacts with a patient throughout a visit should be taking notes on patient preferences and needs. A patient who is squeamish around needles should never have to tell us this more than once.
- Be an agent, not a gatekeeper. “An agent makes things happen for others. A gatekeeper sets up barriers to keep people out.”¹⁴ If a patient has a good reason to be asking you to break one of our rules, and you have a way to break it (within the bounds of the law, obviously), then just break it.
- Surprise and delight. How can you make this the best interaction of someone’s day? Don’t limit your creativity to the confines of a traditional doctor’s office. If a patient is spending a part of her actual birthday at the doctor’s office, there’s no reason we can’t get some balloons involved.
This is the kind of doctor’s office that would flip my switch — one that would give me a very different set of reasons to be a doctor’s pet.
Above all else, healthcare hospitality treats people the way they deserve to be treated. When patients come to us, whether we’re preventing, managing, or treating, the stakes are inherently high. Too high for patients to get worse service than they would at a restaurant. If there’s ever a time to go for the A+, this is it.
To read more about The Lanby, check out Chloe’s companion piece: My Fight with Breast Cancer Drove Me to Fix Primary Care.
Sources
- Customer First Healthcare,” Bill Gurley, Above the Crowd.
- Employer-based health care was a wartime accident, Stephen Mihm, The Chicago Tribune.
- Customer First Healthcare,” Bill Gurley, Above the Crowd. (“While it seems normal to us, the use of the employer as a key constituent in providing consumer healthcare coverage is quite rare and not used in any other industrialized nation.”)
- Direct Primary Care is the future of health, Nick Soman, Medium.
- Customer First Healthcare,” Bill Gurley, Above the Crowd.
- Patients’ №1 complaint? Front-desk staff, Kelly Gooch, Becker’s Hospital Review.
- How long are new patients waiting to see a doctor?, Erin Dietsche, MedCity News.
- For millennials, a regular visit to the doctor’s office is not a primary concern, Sandra G. Goodman, The Washington Post. (“A recent report in JAMA Internal Medicine found that nearly half of patients who sought treatment at an urgent care clinic for a cold, the flu or a similar respiratory ailment left with an unnecessary and potentially harmful prescription for antibiotics, compared with 17 percent of those seen in a doctor’s office.”)
- Time Allocation in Primary Care Office Visits, NCBI.
- Don’t Visit Your Doctor in the Afternoon, Jeffrey A. Linder, The New York Times.
- Up to 40 percent of annual deaths from each of five leading US causes are preventable, CDC.
- Primary care physicians and specialists as personal physicians, NCBI. (Patients with a PCP spend 33% less on healthcare, and experience lower mortality rates than those who only see specialists.)
- Setting The Table, Danny Meyer.
- Setting The Table, Danny Meyer.
